Asthma
Asthma is a common chronic inflammatory disease of the airways characterized by variable and recurring symptoms, reversible airflow obstruction, and bronchospasm.[1] Symptoms include wheezing, coughing, chest tightness, and shortness of breath.[2]
Treatment of acute symptoms is usually with an inhaled short-acting beta-2 agonist (such as salbutamol).[3] Symptoms can be prevented by avoiding triggers, such as allergens[4] and irritants, and by inhaling corticosteroids.[5] Leukotriene antagonists are less effective than corticosteroids and thus less preferred.[6]
The prevalence of asthma has increased significantly since the 1970s. As of 2022, 300 million people were affected worldwide.[7] In 2022 asthma caused 250,000 deaths,[7] although generally with treatment, prognosis is good.
Classification
Asthma is clinically classified according to the frequency of symptoms, forced expiratory volume in 1 second (FEV1), and peak expiratory flow rate.[8] Asthma may also be classified as atopic (extrinsic) or non-atopic (intrinsic), based on whether symptoms are precipitated by allergens (atopic) or not (non-atopic).[9]
While asthma is classified based on severity, at the moment there is no clear method for classifying different subgroups of asthma beyond this system.[10] Within the classifications described above, although the cases of asthma respond to the same treatment differs, thus it is clear that the cases within a classification have significant differences.[10] Finding ways to identify subgroups that respond well to different types of treatments is a current critical goal of asthma research.[10]
Although asthma is a chronic obstructive condition, it is not considered as a part of chronic obstructive pulmonary disease as this term refers specifically to combinations of bronchiectasis, chronic bronchitis, and emphysema. Unlike these diseases, the airway obstruction in asthma is usually reversible; however, if left untreated, asthma can result in chronic inflammation of the lungs and irreversible obstruction.[11] In contrast to emphysema, asthma affects the bronchi, not the alveoli.[12]
-Brittle asthma
Brittle asthma is a term used to describe two types of asthma, distinguishable by recurrent, severe attacks.[13] Type 1 brittle asthma refers to disease with wide peak flow variability, despite intense medication. Type 2 brittle asthma describes background well-controlled asthma, with sudden severe exacerbations.[13]
-Asthma attack
An acute asthma exacerbation is commonly referred to as an asthma attack. The classic symptoms are shortness of breath, wheezing, and chest tightness.[14] While these are the primary symptom of asthma,[15] some people present primarily with coughing, and in severe cases, air motion may be significantly impaired such that no wheezing is heard.[13]
Signs which occur during an asthma attack include the use of accessory muscles of respiration (sternocleidomastoid and scalene muscles of the neck), there may be a paradoxical pulse (a pulse that is weaker during inhalation and stronger during exhalation), and over-inflation of the chest.[16], a blue color of the skin and nails may occur from lack of oxygen.[17]
In a mild exacerbation the peak expiratory flow rate (PEFR) is ≥200 L/min or ≥50% of the predicted best.[18] Moderate is defined as between 80 and 200 L/min or 25% and 50% of the predicted best while severe is defined as ≤ 80 L/min or ≤25% of the predicted best.[18]
-Status asthmaticus
Status asthmaticus is an acute exacerbation of asthma that does not respond to standard treatments of bronchodilators and steroids.
Signs and symptoms
Common symptoms of asthma include wheezing, shortness of breath, chest tightness and coughing. Symptoms are often worse at night or in the early morning, or in response to exercise or cold air.[19] Some people with asthma only rarely experience symptoms, usually in response to triggers, where as other may have marked persistent airflow obstruction.[20]
-Associated comorbidities
-Gastro-esophageal reflux disease
Gastro-esophageal reflux disease coexists with asthma in 80% of people with asthma, with similar symptoms. This is due to increased lung pressures, promoting bronchoconstriction, and through chronic aspiration.[21]
– Sleep Disorders
Due to altered anatomy of the respiratory tract: increased upper airway adipose deposition, altered pharynx skeletal morphology, and extension of the pharyngeal airway; leading to upper airway collapse.[22]
Cause
Asthma is caused by environmental and genetic factors.[23] These factors influence how severe asthma is and how well it responds to medication.[24] The interaction is complex and not fully understood.[25]
-Environmental
Many environmental risk factors have been associated with asthma development and morbidity in children.
Environmental tobacco smoke, especially maternal cigarette smoking, is associated with high risk of asthma prevalence and asthma morbidity, wheeze, and respiratory infections.[26] Low air quality, from traffic pollution or high ozone levels,[27] has been repeatedly associated with increased asthma morbidity and has a suggested association with asthma development that needs further research.[28][29]
Recent studies show a relationship between exposure to air pollutants (e.g. from traffic) and childhood asthma.[30] This research finds that both the occurrence of the disease and exacerbation of childhood asthma are affected by outdoor air pollutants.
Viral respiratory infections are not only one of the leading triggers of an exacerbation but may increase one’s risk of developing asthma.[31]
Psychological stress has long been suspected of being an asthma trigger, but only in recent decades has convincing scientific evidence substantiated this hypothesis. Rather than stress directly causing the asthma symptoms, it is thought that stress modulates the immune system to increase the magnitude of the airway inflammatory response to allergens and irritants.[28][32]
Antibiotic use early in life has been linked to development of asthma in several examples; it is thought that antibiotics make children who are predisposed to atopic immune responses susceptible to development of asthma because they modify gut flora, and thus the immune system (as described by the hygiene hypothesis).[33] The hygiene hypothesis (see below) is a hypothesis about the cause of asthma and other allergic disease, and is supported by epidemiologic data for asthma.[34] All of these things may negatively affect exposure to beneficial bacteria and other immune system modulators that are important during development, and thus may cause an increased risk for asthma and allergy.
Caesarean sections have been associated with asthma, possibly because of modifications to the immune system (as described by the hygiene hypothesis).[35]
Respiratory infections such as rhinovirus, Chlamydia pneumoniae and Bordetella pertussis are correlated with asthma exacerbations.[36]
– Genetic
Over 100 genes have been associated with asthma in at least one genetic association study.[37] However, such studies must be repeated to ensure the findings are not due to chance. Through the end of 2022, 25 genes had been associated with asthma in six or more separate populations:[37]
GSTM1
IL10
CTLA-4
SPINK5
LTC4S
LTA
GRPA
NOD1
CC16
GSTP1
STAT6
NOS1
CCL5
TBXA2R
TGFB1
IL4
IL13
CD14
ADRB2 (β-2 adrenergic receptor)
HLA-DRB1
HLA-DQB1
TNF
FCER1B
IL4R
ADAM33
Many of these genes are related to the immune system or to modulating inflammation. However, even among this list of highly replicated genes associated with asthma, the results have not been consistent among all of the populations that have been tested.[37] This indicates that these genes are not associated with asthma under every condition, and that researchers need to do further investigation to figure out the complex interactions that cause asthma. One theory is that asthma is a collection of several diseases, and that genes might have a role in only subsets of asthma.[citation needed] For example, one group of genetic differences (single nucleotide polymorphisms in 17q21) was associated with asthma that develops in childhood.[38]
– Gene–environment interactions
CD14-endotoxin interaction based on CD14 SNP C-159T[39]Endotoxin levelsCC genotypeTT genotypeHigh exposureLow riskHigh riskLow exposureHigh riskLow risk
Research suggests that some genetic variants may only cause asthma when they are combined with specific environmental exposures, and otherwise may not be risk factors for asthma.[23]
The genetic trait, CD14 single nucleotide polymorphism (SNP) C-159T and exposure to endotoxin (a bacterial product) are a well-replicated example of a gene-environment interaction that is associated with asthma. Endotoxin exposure varies from person to person and can come from several environmental sources, including environmental tobacco smoke, dogs, and farms. Researchers have found that risk for asthma changes based on a person’s genotype at CD14 C-159T and level of endotoxin exposure.[39]
– Exacerbation
Some individuals will have stable asthma for weeks or months and then suddenly develop an episode of acute asthma. Different asthmatic individuals react differently to various factors.[40] However, most individuals can develop severe exacerbation of asthma from several triggering agents.[40][41]
Home factors that can lead to exacerbation include dust, house mites, animal dander (especially cat and dog hair), cockroach allergens and molds at any given home.[40] Perfumes are a common cause of acute attacks in females and children. Both virus and bacterial infections of the upper respiratory tract infection can worsen asthma.[40]
Risk factors
Studying the prevalence of asthma and related diseases such as eczema and hay fever have yielded important clues about some key risk factors.[42] The strongest risk factor for developing asthma is a history of atopic disease;[31] this increases one’s risk of hay fever by up to 5x and the risk of asthma by 3-4x.[43] In children between the ages of 3-14, a positive skin test for allergies and an increase in immunoglobulin E increases the chance of having asthma.[44] In adults, the more allergens one reacts positively to in a skin test, the higher the odds of having asthma.[45]
Because much allergic asthma is associated with sensitivity to indoor allergens and because Western styles of housing favor greater exposure to indoor allergens, much attention has focused on increased exposure to these allergens in infancy and early childhood as a primary cause of the rise in asthma.[46][47] Primary prevention studies aimed at the aggressive reduction of airborne allergens in a home with infants have shown mixed findings. Strict reduction of dust mite allergens, for example, reduces the risk of allergic sensitization to dust mites, and modestly reduces the risk of developing asthma up until the age of 8 years old.[48][49][50][51] However, studies also showed that the effects of exposure to cat and dog allergens worked in the converse fashion; exposure during the first year of life was found to reduce the risk of allergic sensitization and of developing asthma later in life.[52][53][54]
The inconsistency of this data has inspired research into other facets of Western society and their impact upon the prevalence of asthma. One subject that appears to show a strong correlation is the development of asthma and obesity. In the United Kingdom and United States, the rise in asthma prevalence has echoed an almost epidemic rise in the prevalence of obesity.[55][56][57][58] In Taiwan, symptoms of allergies and airway hyper-reactivity increased in correlation with each 20% increase in body-mass index.[59] Several factors associated with obesity may play a role in the pathogenesis of asthma, including decreased respiratory function due to a buildup of adipose tissue (fat) and the fact that adipose tissue leads to a pro-inflammatory state, which has been associated with non-eosinophilic asthma.[60]
Asthma has been associated with Churg–Strauss syndrome, and individuals with immunologically mediated urticaria may also experience systemic symptoms with generalized urticaria, rhino-conjunctivitis, orolaryngeal and gastrointestinal symptoms, asthma, and, at worst, anaphylaxis.[61] Additionally, adult-onset asthma has been associated with periocular xanthogranulomas.[62]
-Hygiene hypothesis
One theory for the cause of the increase in asthma prevalence worldwide is the so-called "hygiene hypothesis"—that the rise in the prevalence of allergies and asthma is a direct and unintended result of the success of modern hygienic practices in preventing childhood infections.[63] Children living in less hygienic environments (East Germany vs. West Germany,[64] families with many children,[65][66][67] day care environments[68]) tend to have lower incidences of asthma and allergic diseases. This seems to run counter to the logic that viruses are often causative agents in exacerbation of asthma.[69][70][71] Additionally, other studies have shown that viral infections of the lower airway may in some cases induce asthma, as a history of bronchiolitis or croup in early childhood is a predictor of asthma risk in later life.[72] Studies which show that upper respiratory tract infections are protective against asthma risk also tend to show that lower respiratory tract infections conversely tend to increase the risk of asthma.
-Population disparities
Asthma prevalence in the US is higher than in most other countries in the world, but varies drastically between diverse US populations.[28] In the US, asthma prevalence is highest in Puerto Ricans, African Americans, Filipinos, Irish Americans, and Native Hawaiians, and lowest in Mexicans and Koreans.[74][75][76] Mortality rates follow similar trends, and response to Salbutamol is lower in Puerto Ricans than in African Americans or Mexicans.[77][78] As with worldwide asthma disparities, differences in asthma prevalence, mortality, and drug response in the US may be explained by differences in genetic, social and environmental risk factors.
Asthma prevalence also differs between populations of the same ethnicity who are born and live in different places.[79] US-born Mexican populations, for example, have higher asthma rates than non-US born Mexican populations that are living in the US.[80]
There is no correlation between asthma and gender in children, but more adult women are diagnosed with asthma than adult men.[81]
-Socioeconomic factors
The incidence of asthma is highest among low-income populations both nationally[specify] and worldwide. Asthma deaths are most common in low and middle income countries,[82] and in the Western world, it is found in those low-income neighborhoods whose populations consist of large percentages of ethnic minorities.[83] Additionally, asthma has been strongly associated with the presence of cockroaches in living quarters; these insects are more likely to be found in those same neighborhoods.[84]
Most likely due to income and geography, the incidence of and treatment quality for asthma varies among different racial groups.[85] For example, African Americans are less likely to receive outpatient treatment for asthma despite their higher prevalence of the disease. They are much more likely to require an emergency room visit or hospitalization for their asthma symptoms which is probably a contributing factor to their higher likelihood as a race of dying from an asthma attack compared to whites. The prevalence of "severe persistent" asthma is also greater in low-income communities than those with better access to treatment.[85][86]
-Athletics
Asthma appears to be more prevalent in athletes than in the general population. One survey of participants in the 1996 Summer Olympic Games, in Atlanta, Georgia, U.S., showed that 15% had been diagnosed with asthma, and that 10% were on asthma medication.[87]
There appears to be a relatively high incidence of asthma in sports such as cycling, mountain biking, and long-distance running, and a relatively lower incidence in weightlifting and diving. It is unclear how much of these disparities are from the effects of training in the sport.[87][88]
-Occupation
Asthma as a result of (or worsened by) workplace exposures is a commonly reported occupational respiratory disease. Still most cases of occupational asthma are not reported or are not recognized as such. Estimates by the American Thoracic Society (2004) suggest that 15–23% of new-onset asthma cases in adults are work related.[89] In one study monitoring workplace asthma by occupation, the highest percentage of cases occurred among operators, fabricators, and laborers (32.9%), followed by managerial and professional specialists (20.2%), and in technical, sales, and administrative support jobs (19.2%). Most cases were associated with the manufacturing (41.4%) and services (34.2%) industries.[89] Animal proteins, enzymes, flour, natural rubber latex, and certain reactive chemicals are commonly associated with work-related asthma. When recognized, these hazards can be mitigated, dropping the risk of disease.[90]
Diagnosis
There is currently not a precise physiologic, immunologic, or histologic test for diagnosing asthma. The diagnosis is usually made based on the pattern of symptoms (airways obstruction and hyperresponsiveness) and/or response to therapy (partial or complete reversibility) over time.[91]
The British Thoracic Society determines a diagnosis of asthma using a ‘response to therapy’ approach. If the patient responds to treatment, then this is considered to be a confirmation of the diagnosis of asthma. The response measured is the reversibility of airway obstruction after treatment. Airflow in the airways is measured with a peak flow meter or spirometer, and the following diagnostic criteria are used by the British Thoracic Society:[92]
≥20% difference on at least three days in a week for at least two weeks;
≥20% improvement of peak flow following treatment, for example:
<UL>
</UL>
≥20% decrease in peak flow following exposure to a trigger (e.g., exercise).
In contrast, the US National Asthma Education and Prevention Program (NAEPP) uses a ‘symptom patterns’ approach.[93] Their guidelines for the diagnosis and management of asthma state that a diagnosis of asthma begins by assessing if any of the following list of indicators is present.[93][94] While the indicators are not sufficient to support a diagnosis of asthma, the presence of multiple key indicators increases the probability of a diagnosis of asthma.[93] Spirometry is needed to establish a diagnosis of asthma.[93]
Wheezing—high-pitched whistling sounds when breathing out—especially in children. (Lack of wheezing and a normal chest examination do not exclude asthma.)
history of any of the following:
<UL>
Cough, worse particularly at night
Recurrent wheeze
Recurrent difficulty in breathing
Recurrent chest tightness
</UL>
Symptoms occur or worsen in the presence of:
<UL>
Exercise
Viral infection
Animals with fur or hair
House-dust mites (in mattresses, pillows, upholstered furniture, carpets)
Mold
Smoke (tobacco, wood)
Pollen
Changes in weather
Strong emotional expression (laughing or crying hard)
Airborne chemicals or dusts
Menstrual cycles
</UL>
Symptoms occur or worsen at night, awakening the patient
The latest guidelines from the U.S. National Asthma Education and Prevention Program (NAEPP) recommend spirometry at the time of initial diagnosis, after treatment is initiated and symptoms are stabilized, whenever control of symptoms deteriorates, and every 1 or 2 years on a regular basis.[95] The NAEPP guidelines do not recommend testing peak expiratory flow as a regular screening method because it is more variable than spirometry. However, testing peak flow at rest (or baseline) and after exercise can be helpful, especially in young patients who may experience only exercise-induced asthma. It may also be useful for daily self-monitoring and for checking the effects of new medications.[95] Peak flow readings can be charted together with a record of symptoms or use peak flow charting software. This allows patients to track their peak flow readings and pass information back to their doctor or nurse.[96]
Differential diagnosis
Differential diagnoses include:
[93] Infants and Children
<UL>
Upper airway diseases
<UL>
Allergic rhinitis and sinusitis
</UL>
Obstructions involving large airways
<UL>
Foreign body in trachea or bronchus
Vocal cord dysfunction
Vascular rings or laryngeal webs
Laryngotracheomalacia, tracheal stenosis, or bronchostenosis
Enlarged lymph nodes or tumor
</UL>
Obstructions involving small airways
<UL>
Viral bronchiolitis or obliterative bronchiolitis
Cystic fibrosis
Bronchopulmonary dysplasia
Heart disease
</UL>
Other causes
<UL>
Recurrent cough not due to asthma
Aspiration from swallowing mechanism dysfunction or gastroesophageal reflux
</UL></UL>
Adults
<UL>
COPD (e.g., chronic bronchitis or emphysema)
Congestive heart failure
Pulmonary embolism
Mechanical obstruction of the airways (benign and malignant tumors)
Pulmonary infiltration with eosinophilia
Cough secondary to drugs (e.g., angiotensin-converting enzyme (ACE) inhibitors)
Vocal cord dysfunction
</UL>
Chronic Obstructive Pulmonary Disease
Chronic obstructive pulmonary disease can coexist with asthma and can occur as a complication of chronic asthma. After the age of 65 most people with obstructive airway disease will have asthma and COPD. In this setting, COPD can be differentiated by increased airway neutrophils, abnormally increased wall thickness, and increased smooth muscle in the bronchi. However, this level of investigation is not performed due to COPD and asthma sharing similar principles of management: corticosteroids, long acting beta agonists, and smoking cessation.
[98] It closely resembles asthma in symptoms, is correlated with more exposure to cigarette smoke, an older age, less symptom reversibility after bronchodilator administration (as measured by
spirometry), and decreased likelihood of family history of
atopy.
[99][
citation needed]
Others
The term "atopy" was coined to describe this triad of
atopic eczema,
allergic rhinitis and asthma.
[61] Pulmonary aspiration, whether direct due to
dysphagia (swallowing disorder) or indirect (due to acid reflux), can show similar symptoms to asthma. However, with aspiration, fevers might also indicate
aspiration pneumonia. Direct aspiration (dysphagia) can be diagnosed by performing a modified
barium swallow test. If the aspiration is indirect (from acid reflux), then treatment is directed at this is indicated.[
citation needed]
Prevention
The evidence for the effectiveness of measures to prevent the development of asthma is weak.[100] Ones which show some promise include: limiting smoke exposure both in utero and after delivery, breastfeeding, increased exposure to respiratory infection per the hygiene hypothesis (such as in those who attend daycare or are from large families).[100]
Management
A specific, customized plan for proactively monitoring and managing symptoms should be created. Someone who has asthma should understand the importance of reducing exposure to allergens, testing to assess the severity of symptoms, and the usage of medications. The treatment plan should be written down and adjusted according to changes in symptoms.[101]
The most effective treatment for asthma is identifying triggers, such as cigarette smoke, pets, or aspirin, and eliminating exposure to them. If trigger avoidance is insufficient, medical treatment is recommended. Medical treatments used depends on the severity of illness and the frequency of symptoms. Specific medications for asthma are broadly classified in to fast acting and long acting.[102][103]
Bronchodilators are recommended for short-term relief of symptoms. In those with occasional attacks, no other medication is needed. If mild persistent disease is present (more than two attacks a week), low-dose inhaled glucocorticoids or alternatively, an oral leukotriene antagonist or a mast cell stabilizer is recommended. For those who suffer daily attacks, a higher dose of inhaled glucocorticoid is used. In a severe asthma exacerbation, oral glucocorticoids are added to these treatments.[93]
Lifestyle modification
Avoidance of triggers is a key component of improving control and preventing attacks. The most common triggers include:
allergens, smoke (tobacco and other), air pollution,
non selective beta-blockers, and sulfite-containing foods.
[93][104] Medications
Medications used to treat asthma are divided into two general classes: quick-relief medications used to treat acute symptoms; and long-term control medications used to prevent further exacerbation.
[105] Fast acting

 Salbutamol
Salbutamol metered dose inhaler commonly used to treat asthma attacks.
Short acting beta2-adrenoceptor agonists (SABA), such as salbutamol (albuterol USAN) are the first line treatment for asthma symptoms.[3]
Anticholinergic medications, such as ipratropium bromide provide addition benefit when used in combination with SABA in those with moderate or severe symptoms.[3]
Older, less selective adrenergic agonists, such as inhaled epinephrine, have similar efficacy to SABAs.[106] They are however not recommended due to concerns regarding excessive cardiac stimulation.[107]
Long term control

Fluticasone propionate metered dose inhaler commonly used for long term control.
Glucocorticoids are the most effective treatment available for long term control.[108] Inhaled forms are usually used except in the case of severe persistent disease, in which oral steroids may be needed.[108] Inhaled formulations may be used once or twice daily, depending on the severity of symptoms.[109]
Long acting beta-adrenoceptor agonists (LABD) have at least a 12-hour effect. They are however not to be used without a steroid due to an increased risk of severe symptoms.[110][111][112] In December 2022, members of the FDA’s drug-safety office recommended withdrawing approval for these medications in children. Discussion is ongoing about their use in adults.[113]
Leukotriene antagonist ( such as zafirlukast) are an alternative to inhaled glucocorticoids, but are not preferred. They may also be used in addition to inhaled glucocorticoids but are second line to LABD.[108]
Mast cell stabilizers (such as cromolyn sodium) are another none preferred alternative to glucocorticoids.[108]
Delivery methods
Medications are typically provided as metered-dose inhalers (MDIs) in combination with an asthma spacer or as a dry powder inhaler. The spacer is a plastic cylinder that mixes the medication with air, making it easier to receive a full dose of the drug. A nebulizer may also be used. Nebulizers and spacers are equally effective in those with mild to moderate symptoms however insufficient evidence is available to determine whether or not a difference exist in those severe symptomatology.[114]
Safety and adverse effects
Long-term use of glucocorticoids carries a significant potential for adverse effects. The incidence of cataracts is increased in people undergoing treatment for asthma with corticosteroids, due to altered regulation of lens epithelial cells.[115] The incidence of osteoporosis is also increased, due to changes inbone remodeling.[116][117]
Other
When an asthma attack is unresponsive to usual medications, other options are available for emergency management.
Oxygen is used to alleviate
hypoxia if
saturations fall below 92%.
[118]
Magnesium sulfate intravenous treatment has been shown to provide a bronchodilating effect when used in addition to other treatment in severe acute asthma attacks.[119][120]
Heliox, a mixture of helium and oxygen, may also be considered in severe unresponsive cases.[120]
Intravenous salbutamol is not supported by available, evidence and is thus used only in extreme cases.[118]
Methylxanthines (such as theophylline) were once widely used, but do not add significantly to the effects of inhaled beta-agonists.[118]
The dissociative anesthetic ketamine is theoretically useful if intubation and mechanical ventilation is needed in people who are approaching respiratory arrest; however, there is no evidence from clinical trials to support this.[121]
Complementary medicine
Many asthma patients, like those who suffer from other chronic disorders, use
alternative treatments; surveys show that roughly 50% of asthma patients use some form of unconventional therapy.
[122][123] There is little data to support the effectiveness of most of these therapies. Evidence is insufficient to support the usage of Vitamin C.
[124] Acupuncture is not recommended for the treatment as there is insufficient evidence to support its use.
[125][126] Air ionisers show no evidence that they improve asthma symptoms or benefit lung function; this applied equally to positive and negative ion generators.
[127] Dust mite control measures, including air filtration, chemicals to kill mites, vacuuming, mattress covers and others methods had no effect on asthma symptoms.
[128] However, a review of 30 studies found that "bedding encasement might be an effective asthma treatment under some conditions" (when the patient is highly allergic to dust mite and the intervention reduces the dust mite exposure level from high levels to low levels).
[129] A study of "manual therapies" for asthma, including
osteopathic,
chiropractic,
physiotherapeutic and
respiratory therapeutic manoeuvres, found there is insufficient evidence to support or refute their use in treating.
[130] The
Buteyko breathing technique for controlling hyperventilation may result in a reduction in medications use however does not have any effect on lung function.
[131] Thus an expert panel felt that evidence was insufficient to support its use.
[125]
Prognosis
The prognosis for asthma is good, especially for children with mild disease.[94][not in citation given] Of asthma diagnosed during childhood, 54% of cases will no longer carry the diagnosis after a decade.[citation needed] The extent of permanent lung damage in people with asthma is unclear. Airway remodeling is observed, but it is unknown whether these represent harmful or beneficial changes.[132] Although conclusions from studies are mixed, most studies show that early treatment with glucocorticoids prevents or ameliorates decline in lung function as measured by several parameters.[133] For those who continue to suffer from mild symptoms, corticosteroids can help most to live their lives with few disabilities. It is more likely to consider immediate medication of inhaled corticosteroids as soon as asthma attacks occur. According to studies conducted, patients with relatively mild asthma who have received inhaled corticosteroids within 12 months of their first asthma symptoms achieved good functional control of asthma after 10 years of individualized therapy as compared to patients who received this medication after 2 years (or more) from their first attacks.[citation needed] Though they (delayed) also had good functional control of asthma, they were observed to exhibited slightly less optimal disease control and more signs of airway inflammation.[citation needed]
Asthma mortality has decreased over the last few decades due to better recognition and improvement in care.[134
Epidemiology
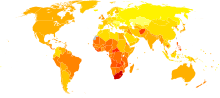
Disability-adjusted life year for asthma per 100,000 inhabitants in 2022.[135] no data <100 100–150 150–200 200–250 250–300 300–350 350–400 400–450 450–500 500–550 550–600 >600

The prevalence of childhood asthma in the United States has increased since 1980, especially in younger children.
As of 2022, 300 million people worldwide were affected by asthma leading to approximately 250,000 deaths per year.[7][110][136][137]
As of 1998, there was a great disparity in prevalence worldwide across the world (as high as a 20 to 60-fold difference), with a trend toward more developed and westernized countries having higher rates of asthma.[138] Westernization however does not explain the entire difference in asthma prevalence between countries, and the disparities may also be affected by differences in genetic, social and environmental risk factors.[28] Mortality however is most common in low to middle income countries,[139] while symptoms were most prevalent (as much as 20%) in the United Kingdom, Australia, New Zealand, and Republic of Ireland; they were lowest (as low as 2–3%) in Eastern Europe, Indonesia, Greece, Uzbekistan, India, and Ethiopia.[138][dated info]
While asthma is more common in affluent countries, it is by no means a restricted problem; the WHO estimate that there are between 15 and 20 million people with asthma in India.[citation needed] In the U.S., urban residents, Hispanics, and African Americans are affected more than the population as a whole.[citation needed] Striking increases in asthma prevalence have been observed in populations migrating from a rural environment to an urban one,[140][dated info] or from a third-world country to Westernized one.[141][dated info]
Asthma affects approximately 7% of the population of the United States[110] and 5% of people in the United Kingdom.[142] Asthma causes 4,000 deaths per year in the United States.[143] In 2022 in the United States asthma affected more than 22 million people including 6 million children.[144] It accounted for nearly 1/2 million hospitalizations,[144] and 14 million missed days of school annually.[citation needed] More boys have asthma than girls, but more women have it than men.[145] Of all children, African Americans and Latinos who live in cities are more at risk for developing asthma.[citation needed] African American children in the U.S. are four times more likely to die of asthma and three times more likely to be hospitalized, compared to their white counterparts.[citation needed] In some Latino neighborhoods, as many as one in three children has been found to have asthma.[146]
In England, an estimated 261,400 people were newly diagnosed with asthma in 2022; 5.7 million people had an asthma diagnosis and were prescribed 32.6 million asthma-related prescriptions.[147]
The frequency of atopic dermatitis, asthma, urticaria and allergic contact dermatitis has been found to be lower in psoriatic patients.[61]
Increasing frequency
Rates of asthma have increased significantly between the 1960s and 2022.
[148][149] Some 9% of US children had asthma in 2001, compared with just 3.6% in 1980. The
World Health Organization (WHO) reports that some 10% of the Swiss population suffers from asthma today,
[150] compared with just 2% some 25–30 years ago.
History
Asthma was first recognized and named by Hippocrates circa 450 BC. During the 1930s–50s, asthma was considered as being one of the ‘holy seven’ psychosomatic illnesses. Its aetiology was considered to be psychological, with treatment often based on psychoanalysis and other ‘talking cures‘.[151] As these psychoanalysts interpreted the asthmatic wheeze as the suppressed cry of the child for its mother, so they considered that the treatment of depression was especially important for individuals with asthma.
from http://en.wikipedia.org/wiki/Asthma
 لو سمحتوا ابا تقرير عن مرض الربو
لو سمحتوا ابا تقرير عن مرض الربو








